Health (DP IB Global Politics: HL): Revision Note

Health in global politics
A set of topic areas is presented for the study of global political challenges to facilitate your explorations. These should not be seen as fully discrete or disconnected topics, but rather as overlapping areas of study that can contribute to understanding and addressing global challenges.
You can conduct an in-depth study of two of the topic areas—for example, security and health—or you may choose to explore the interconnections of multiple topic areas based on a selected case study.
Health is a fundamental human right and a central dimension of human security
Global health challenges are inherently political - they involve questions of resource allocation, sovereignty, inequality and international cooperation
Health operates at every level - global (international frameworks and organisations such as the WHO), regional (cross-border surveillance and shared responses), national (state health systems and public health policy) and local (community outcomes and inequalities within populations)
The political fault lines on health tend to run between states with very different health-system capacity, and between groups within states whose access to care is shaped by income, gender, ethnicity and geography
Why health is a global political challenge
Infectious diseases spread across borders regardless of political policy
No state can fully protect its population through unilateral action
Global health is deeply connected to inequality
Poorer states and communities face greater health burdens with fewer resources to address them
Health systems are inherently political
Decisions about who receives healthcare, which diseases receive funding and how health emergencies are managed reflect power relations within and between states
The tension between state sovereignty and international health governance is a central challenge
States may resist international oversight of their health systems, even during emergencies
Health emergencies can destabilise states by overwhelming services, disrupting economies and undermining political legitimacy
Key terms and concepts
Term | Definition |
|---|---|
Pandemic |
|
Epidemic |
|
World Health Organisation (WHO) |
|
Social determinants of health |
|
Health equity |
|
Universal health coverage (UHC) |
|
Public Health Emergency of International Concern (PHEIC) |
|
Non-communicable disease (NCD) |
|
Humanitarian health response |
|
Types of health challenge
1. Infectious and epidemic disease
Diseases caused by pathogens (viruses, bacteria) that spread between people - historically the most significant cause of premature death globally
Epidemics spread rapidly within a specific population or region; pandemics spread across multiple countries or continents
International cooperation is essential for containing epidemic disease, but states may prioritise national interests over collective action
2. Non-communicable diseases (NCDs)
Chronic conditions - heart disease, cancer, diabetes, respiratory disease - are now the leading cause of death globally
Shaped by lifestyle, environment, poverty and inequality
Receive less international attention than infectious diseases despite causing more deaths - partly because they are perceived as individual rather than political problems
3. Structural health inequalities
Systematic differences in health outcomes between groups, driven by poverty, discrimination, geography and unequal access to healthcare
The social determinants of health are the primary driver of health inequalities (see Key Framework below)
These are political, not natural: they reflect decisions about resource allocation, land, labour and governance
4. Health in conflict and displacement
Armed conflict destroys health infrastructure, forces health workers to flee and cuts off access to medicines and treatment
Refugee camps and displacement settings are associated with infectious disease, malnutrition and severe mental health challenges
International humanitarian law requires the protection of health facilities in conflict - in practice, this rule is frequently violated
A useful analytical lens: the social determinants of health
One of the most productive ways to read a health case study is through the social determinants framework - particularly any case where unequal health outcomes need to be explained, or where political and economic factors are shaping who gets sick and who has access to care. It won't be the right lens for every case, but it has analytical traction on most of them.
The social determinants of health are the non-medical factors that shape health outcomes - the conditions in which people are born, grow, live, work and age.
They were formally defined by the WHO Commission on Social Determinants of Health (2008), chaired by Sir Michael Marmot. The Commission concluded that the conditions of daily life are responsible for a large proportion of health inequalities - and that these conditions are themselves the result of political choices.
Key social determinants
Income and wealth - poverty is the single strongest predictor of poor health; wealthier individuals and states live longer and experience better health outcomes
Education - higher levels of education correlate strongly with better health literacy, safer working conditions and greater access to healthcare
Housing and environment - overcrowded or unsanitary housing increases the risk of infectious disease; proximity to pollution damages respiratory health
Gender - women and girls face specific health risks related to reproductive health, gender-based violence and unequal access to healthcare
Ethnicity and race - racial discrimination affects health both directly (through stress and violence) and indirectly (through reduced access to education, employment and healthcare)
Why it matters in global politics
Health cannot be separated from questions of poverty, inequality, governance and human rights
Improving health outcomes requires political action well beyond the health sector - on wages, housing, education and discrimination
States and international organisations that focus only on medical interventions (drugs, vaccines, hospitals) without addressing underlying social conditions will achieve limited results
The framework challenges the idea that individual behaviour is the primary driver of health - it shifts responsibility towards political actors and structures
A useful process model: the political cascade of a health crisis
A health crisis rarely remains a purely medical event - it often triggers a cascade of political, economic and social consequences
Where this dynamic is at work, tracing the cascade below shows how a health shock ripples through the political system
It pairs naturally with the social determinants framework - social determinants explain why certain populations are exposed to health risks in the first place, the cascade explains how a health crisis ripples outwards once it takes hold
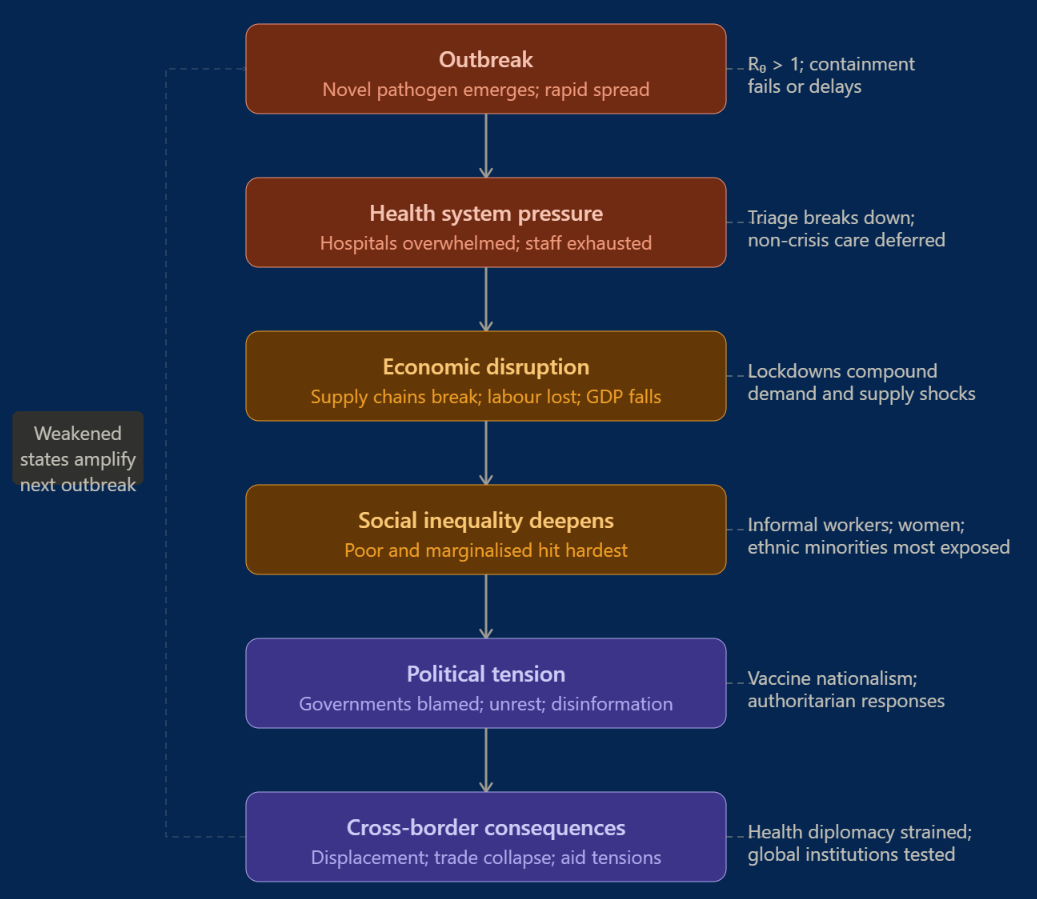
Outbreak concentrates attention on the immediate threat
Health systems are overwhelmed; routine care for other conditions is suspended
The political pressure on governments to act is intense, but the scientific picture is often uncertain
States with weaker health infrastructure are exposed — their capacity to govern effectively is called into question
Economic disruption follows as workers fall ill, supply chains break down and businesses close
Tax revenues fall precisely when demands on the state rise — for emergency health spending, social protection and economic support
Poorer states cannot borrow at the same rates as wealthier ones; the economic cost of a health crisis is therefore distributed unequally
Social consequences deepen existing inequalities
Those in informal employment, without savings or without access to digital services suffer most
Marginalised communities — ethnic minorities, women, the elderly — are disproportionately affected both by the disease itself and by the policy response
Stigma and discrimination frequently attach to affected groups, generating human rights concerns
State responses create their own political tensions
Emergency powers - lockdowns, quarantine, surveillance - restrict civil liberties
The legitimacy of these measures depends on public trust; where trust is low, compliance is low and the effectiveness of the response is undermined
Authoritarian governments have used health emergencies to justify measures that extend beyond public health into political control
Cross-border consequences close the loop
Border closures disrupt trade, migration and remittances
Competition for scarce resources (vaccines, personal protective equipment) exposes the limits of international cooperation
Lower-income states are consistently last to receive the tools they need, reinforcing the structural inequalities that made them vulnerable in the first place
This is what distinguishes a health crisis from a contained medical event - the cascade it triggers reaches every dimension of political life, and the states least equipped to manage it bear the greatest cost
Current and recent health challenges
Health challenges in the contemporary world take many forms and affect states at every level of development.
Pandemics - cross-border disease spread that overwhelms state capacity (e.g. COVID-19 from 2020)
HIV/AIDS - a long-running global epidemic, with approximately 25 million cases in Africa
Non-communicable diseases - heart disease, cancer and diabetes, now the top cause of death globally
Mental health - chronically underfunded with a growing burden, particularly in displacement settings (e.g. PTSD among Syrian refugees)
Actors and stakeholders
When researching a case study on health, students should identify a range of actors and stakeholders:
Nation-states
Set national health policy and allocate healthcare resources
Negotiate international health agreements and contribute to the WHO
May resist international oversight of their health systems, even in emergencies
The World Health Organization (WHO)
The primary UN agency for international public health
Declares Public Health Emergencies of International Concern (PHEICs)
Has no enforcement powers - can coordinate and advise but cannot compel states to act
Non-governmental organisations (NGOs)
E.g. Medecins Sans Frontieres (MSF), which provides medical care in conflict zones and crisis settings
Often operate where state health systems have collapsed or are inaccessible
Pharmaceutical companies
Develop and manufacture medicines and vaccines
Their pricing decisions and intellectual property protections determine who can access essential treatments globally
International financial institutions
E.g. the World Bank and IMF, which provide financing for health systems in lower-income states
Their conditions for lending have historically required reductions in public spending, including on health
Social movements and patient advocacy groups
Campaign for access to medicines, research funding and equitable health policy
E.g. the Treatment Action Campaign in South Africa, which successfully challenged pharmaceutical patents on HIV/AIDS drugs
Civilian populations
Those most directly affected by health policy decisions
Health outcomes vary dramatically by class, gender, ethnicity and geography within as well as between states
Example case studies
The following examples illustrate the kinds of case studies students could develop for this topic area
Case study | Outline | Connections to other HL topics |
|---|---|---|
The 2014-2015 Ebola outbreak in Liberia |
|
|
HIV/AIDS in rural South Africa |
|
|
Syrian refugees and healthcare in Jordan |
|
|
Links to earlier course content
The health topic area connects to all four areas of the IB Global Politics course
Section | Key connections |
|---|---|
Core topics |
|
Rights and justice |
|
Development and sustainability |
|
Peace and conflict |
|
Links to the other HL topic areas
A case study on health will frequently connect to other HL topic areas - identifying these links is essential for question 3
HL topic area | Key connections |
|---|---|
Security |
|
Equality |
|
Identity |
|
Environment |
|
Poverty |
|
Borders |
|
Examiner Tips and Tricks
What distinguishes top-band answers is the deployment of named analytical concepts rather than description alone.
The social determinants of health is one strong lens for many health cases - when applying it, consider how poverty, inequality or discrimination shape the health outcomes of the people involved. The political cascade of a health crisis is a useful complement: strong answers don't just describe a health event but trace it through outbreak, economic disruption, social consequences, state response and cross-border consequences.
The syllabus also rewards drawing on the four core concepts (power, sovereignty, legitimacy, interdependence), broader theoretical perspectives (realism, liberalism, cosmopolitanism), levels of analysis (local to global) and multiple stakeholder perspectives. The right concept depends on your specific case - and many cases reward more than one.

Unlock more, it's free!
Join the 100,000+ Students that ❤️ Save My Exams
the (exam) results speak for themselves:

Was this revision note helpful?
